 blog.gov.je
blog.gov.jeThe following speech was given by the Minister for Infrastructure, Deputy Tom Binet, to members of the Jersey Chamber of Commerce at a Breakfast Briefing on Monday 26th June 2023:
Good morning, everyone, and thank you for taking the time to turn up at this early hour, to hear Ian and me talk about the new hospital facilities.
And thank you, Murray, and the Chamber of Commerce, for hosting this special briefing.
Given the composition of this audience, I’ve taken the liberty of assuming that most of you will have followed the hospital saga over the past decade. Or, at least, you’ll be familiar with the more recent ‘Our Hospital’ scheme, developed by the last government.
On a personal level, I’d been critical about several aspects of the ‘Our Hospital’ scheme before the last election. But whatever my thoughts might have been (or anyone else’s for that matter), it was clear by the time we came to office, that the project needed serious reconsideration.
And that was simply due to the dramatic global changes we’d seen, particularly the effects of the war in Ukraine.
One of the first things that became apparent to us all was that the planned funding mechanism for the ‘Our Hospital’ scheme was completely broken.
The billion-pound strategic investment fund that we’d been told (perhaps rather naively), would deliver 4.5% interest for 40 years, against borrowings of half that cost, simply wasn’t going to deliver. In fact, the picture was quite grim.
Interest rates had already doubled (and were set to increase further), before the Planning Permit materialised, or any borrowing could be put in place.
Finally, when the cost estimates were updated a few weeks later, the construction (and contingency) costs had already risen from the originally quoted £804 million, to £970 million.
Against such a volatile background, it just didn’t seem sensible to commit to a project that looked highly likely to exceed £1 billion, all in one go.
So that was our starting point, but it wasn’t the only factor.
We had to confront the fact that the hospital plan we inherited was designed around the incoherent and undeliverable ‘Jersey Care Model’; treating large numbers of patients in their own homes.
This ill-conceived idea was already in its death-throes, but its demise left us to deal with the fact that the ‘Our Hospital’ plans lacked many of the facilities, and bed numbers, needed to deliver the services we required.
Having watched two successive governments trying to cram twice as much development on a site as it could accommodate (firstly at Gloucester Street, and more recently at Overdale), it seemed logical to consider dividing the main facility over those two (closely situated) sites.
And it was against this background that the Council of Ministers embarked upon a 100-day review; an exercise co-ordinated by the very capable and experienced Northern Irelander, Mr Alan Moore.
The final report, endorsed by him in November 2022, confirmed that our ideas had real potential, and this resulted in us obtaining the necessary funds from the States Assembly, last December, to progress the outlined programme through 2023.
Following that, our excellent Programme team set about producing a Feasibility Study to understand what could be delivered at Overdale and Kensington Place, whilst ensuring the best, and safest, outcomes for patients, clinicians, and hospital workers.
That Feasibility Study, which was completed a short while ago, involved a substantial amount of analytical work and a comprehensive consultation process, to define which parts of the hospital’s functions could be co-located to best effect.
It drew on all the information accumulated from all the previous hospital schemes, ensuring we’re still getting some value, from the money that’s already been spent.
Most importantly, that split of services was decided by way of engagement with a whole range of clinicians, nurses, medical practitioners, and technical health staff.
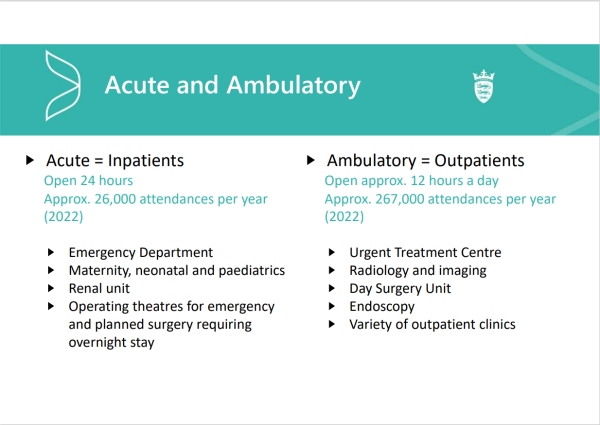
They told us that the most workable split would be between Acute services and Ambulatory services. In layman’s terms, Inpatients and Outpatients.
The team examined Overdale, and the area around Kensington Place, in detail, to see what scale of development each site could accommodate.
They found that both sites could provide the area needed to deliver the larger of the two functions – the acute hospital, at around 45,000m2.
We also asked the team to consider the possibility of developing a health village in the area of St Saviour’s Hospital, to provide an eastern hub, and a range of therapeutic and outpatient services, alongside mental health care.
This achieves the desire to combine mental and physical services on one site, without Mental Health patients feeling they have to use the services of a ‘hospital’; quite an important point for anyone familiar with the many difficulties associated with Mental Illness.
Anyway, from all that work, two Options were put forward for evaluation.
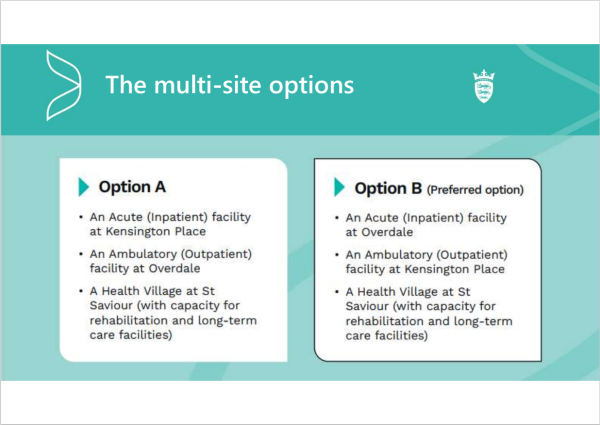
Option A – which puts the Acute (or inpatient) hospital at Kensington Place/Gloucester Street, and the Ambulatory (or outpatients) facility at Overdale, supported by the St Saviour’s Health Village.
And Option B – the direct opposite. With an Inpatient Hospital at Overdale, Outpatient facilities on Kensington Place/Gloucester Street and, again, a Health Village at St Saviour.
The evaluation itself was a pretty comprehensive exercise. Over a three-day period, a series of five panel sessions took place (independently chaired by Crown Advocate Cyril Whelan), examining the clinical, locational, environmental, economic, social and construction aspects of each option.
The outcomes couldn’t have been clearer, and beyond providing an obvious option for us to take forward, they emphasised that the multi-site approach offered a series of benefits that the single ‘Our Hospital’ project simply couldn’t deliver.
Most critically, it provides a plan for the development of an entire healthcare estate, ensuring those services that were not contained in the ‘Our Hospital’ scheme are now provided; and in an appropriate location.
This includes delivery an additional 134 beds across the three sites, as well as a range of services, like hydrotherapy, physiotherapy, dementia care and rehabilitation. In total, that’s 30,000m2 of additional area.
And, unlike the development of the single-site, single-phase ‘Our Hospital’ building, the multi-site, phased approach, doesn’t place all the financial, or construction risk, into one huge project, with one powerful delivery partner.
Notwithstanding that we will need some form of external partner, at some point, our approach (with a series of projects delivered in smaller phases), will certainly provide better opportunities for local construction companies, be that for demolition, base works, M&E or the construction itself.
And given the greatly improved ratio of build volume to site area, it also provides a great opportunity for future expansion on all sites. That’s a very desirable component that couldn’t be achieved with the ‘Our Hospital’ proposal.
As you’ll see in a moment, this solution doesn’t require substantial changes to Westmount Road, or the demolition of Westmount Terrace, the destruction of the Jersey Bowls Club or the utilisation of Warwick Farm for its replacement. Quite a saving, if you add it all up!
This is possible because of the predicted reduction in traffic movements to the Overdale site, caused by the separation of inpatient and outpatient services.
Indeed, the traffic reduction with Option B, is such that it wouldn’t require the construction of the expensive, and unsightly, multi-storey car park, which the Our Hospital plan had in store for Overdale.
A multi-site development also creates additional public space around the old, listed, hospital building on Gloucester Street, and both options allow for the large 1980s building to be transferred to other uses, the most obvious being Key Worker Accommodation.
And, crucially, for many Islanders, the use of both sites will reduce the physical mass on each of them, lowering the impact on both the natural, and the built environment. As a result, we’ll end up with buildings set in much better proportion to their surroundings.
So, if you haven’t already guessed, the option that came out best in the evaluation process was Option B; Inpatients at Overdale and Outpatients at Kensington Place/Gloucester Street.
Perhaps most importantly, Option B scored significantly higher in the evaluation by Clinicians, who rated it ‘Very Good’, as opposed to ‘Adequate’ for Option A. That clinical evaluation is critical, so it must be central to our decision making process.
Equally important to clinicians was the fact that the construction timetable for Option B will give us an operational Acute hospital by 2028; that’s four years earlier than could be achieved if we adopted Option A.
Given that the Inpatient facility requires much more area than the Outpatients, and the Overdale site is a lot larger than the area available at Gloucester Street/Kensington Place, Option B uses both sites to their best possible potential.
It optimises space for the use of Modern Methods of Construction, and minimises delay in construction, due to the better ratio between build volume and site size.
Option B also eliminates the impact of construction work on sick patients. In this instance, all construction work on the Acute (or Inpatient) hospital at Overdale would be devoid of any nearby hospital activity, throughout the entire process.
Whereas Option A, (the construction of an Acute unit at Gloucester Street/Kensington Place) would have to be undertaken right next to a functioning General Hospital, the Acute section of which would still be in full operation.
Overdale also provides the opportunity for better, and more efficient, clinical adjacencies – due to the larger size of the site.
Fortunately, almost 90% of the total patient footfall into the existing hospital relates to ‘Outpatient’ and ‘day-care’ activity.
With Option B, all this will remain in town, with much easier pedestrian access, better public transport, and parking. It would also include access to an Urgent Treatment Centre (that’s the ‘walk in’ part of the current A&E).
Option B also provides peaceful treatment and recovery space for inpatients at Overdale, with increased privacy and much better views than a town location.
Finally, it provides a more balanced opportunity for future expansion on both sites, when compared to Option A.
If you look at screen, you’ll see some images.
It’s important to note that these aren’t finished plans, or final designs. They’re not even close to what the hospital buildings might, eventually, look like.
But they are part of the work the team has done to gauge just what the required volume of development might look like on each site.
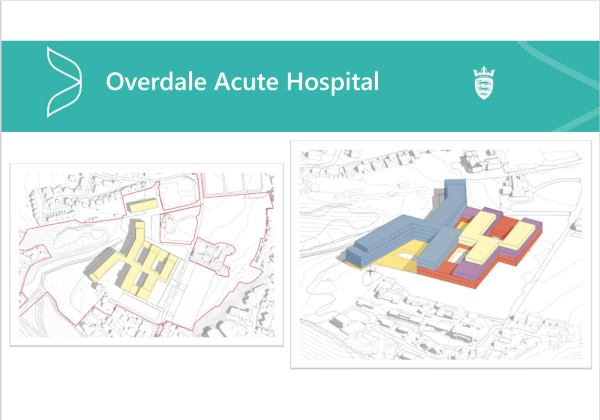
The first is the Acute Hospital at Overdale.
At 48,000m2 it’s one third smaller than the Our Hospital plan. It doesn’t cross Westmount Road, or require the demolition of any of the neighbouring properties.
And even at its highest point, it’s at least one medical storey (that’s one and a half normal stories) lower than the ‘Our Hospital’ Plans.
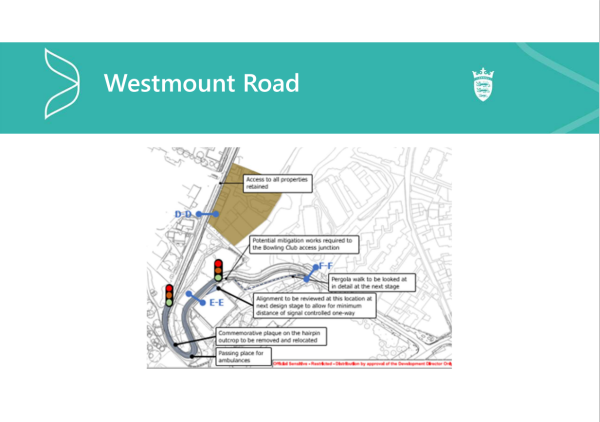
The preservation of Westmont Road is important to this plan, as the whole team has been very committed to avoid spending many millions of pounds on changing the road layout, whilst making sure that ambulances can still come and go safely.
To achieve this, they’ve worked with I&E, the Parish of St Helier Roads Committee, and the Ambulance Service, to come up with a plan.
Sometimes the simplest solutions can deliver what’s needed. And a proposal to install a set of traffic-lights at the hairpin bend, designed to give priority to ambulances at all times, has been welcomed by all concerned.
Work still needs to be done to test this out, but it’s a practical, simple solution, that I think, makes sense.

Kensington Place (as you’ll see on the screen), could provide 25,000m2 of outpatient facilities. This would be a phased development as part of the ongoing healthcare estate plan.
It releases space on the site to be a public park (or gardens of some description), and it reconnects Kensington Place and Gloucester Street.
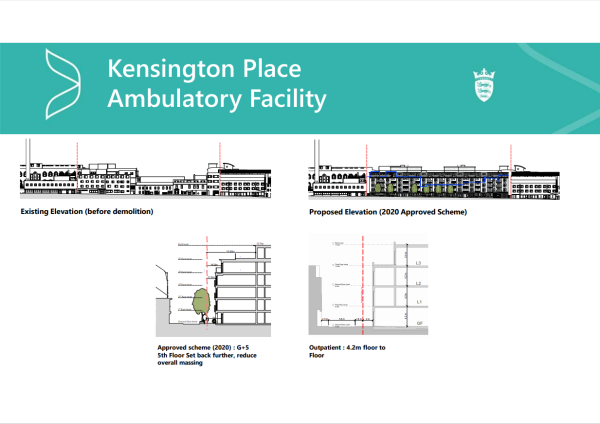
From the outset, the team has worked hard to ensure that the height of any proposal to build in Kensington Place would not exceed the hight granted to Andium in its 2020 Planning Application.

In both A & B schemes, the plan for the St Saviour health Village (adjacent to Clinque Pinel), is pretty much the same. It’s a beautiful, private, location and it’s ideal for assisting the wellbeing and recovery of all those who’ll get to use it.
It’ll also play a vital role in reducing the stigma associated with mental health services, by becoming a shared home for physical healthcare delivery, including physiotherapy and hydrotherapy.
And, of real importance to the many Islanders who’ve suffered the horrors of a stroke (and the families who’ve cared for them), the St Saviour site provides an ideal location for a new rehabilitation unit, to replace the ‘Samares Ward’.
I saw, first hand, the damaging consequences of closing it during Covid, for whatever reason they offered up. And I intend to make absolutely sure that we have an interim facility of no lessor quality, to use between the closure of the old ward and the opening of the new one.
The final piece of the healthcare estate is the one that’ll be delivered first.
The ‘Enid Quenault Health and Wellbeing Centre’ will open this Summer, at the old Les Quennevais School site.
The Chief Minister herself toured the site on Friday, and I hope she’ll agree with me that it can provide a fantastic, and long-term home for a good number of services.
And having spent £15 million there, it makes sense that we should get more long-term value from the investment.
It’ll be the new location for many of the services currently at Overdale, including the Child Development Centre, which will occupy facilities quite a lot larger than the ones they have now.
And (just as a word of reassurance), we’re not looking to move staff, or patients, without clear notice, and assistance. And the team will be doing all they can to ensure that transport and parking is in place, without hampering local residents.
We’ll also make sure that clinicians are supported as they transfer their services. I should also mention that, just because a service is moving out west now, doesn’t mean it will stay there indefinitely, especially if it could be better delivered from any of the other sites – once they’re ready.
So, where do we go next?
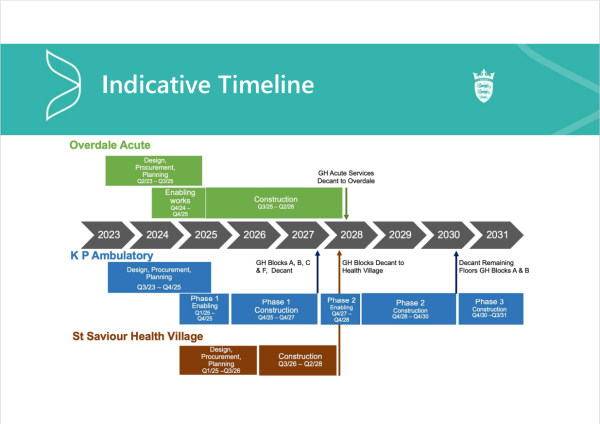
The team has put together a timeline that allows work to begin in earnest at Overdale, whilst taking the first steps to establish the wider estate plan.
This is a ‘programme’ of work, and it consists of a number of projects. And it has the flexibility to stretch or contract them, to meet the economic needs of the moment.
But our Priority is, and must be, the delivery of an acute hospital facility in the next four years.
I hope you’ll agree with me (and the many people we’ve engaged with in recent weeks), that this overall plan is one that makes sense. In my view, it’s got a great deal to commend it.
We’ll be presenting the final Feasibility Study to the States Assembly in July, and from there we’ll be looking to take Option B (the preferred option), forward for design.
I’m calling it the preferred option, but, in reality, it’s the ONLY option.
That’s because it’s the one that delivers the acute hospital that we desperately need, in an acceptable timeframe, with as many benefits as it’s possible to achieve, under the circumstances.
The plan may not please everyone. But after 10 long years, if we can spread the lowest possible level of discontent, over the widest possible area, we may, finally, get the facilities we need, in the sequence that they’re most needed, without pushing the island over the edge of a financial cliff.
We have a really super team of experienced locals heading this up. They’re making very swift progress, using all the information gathered in previous schemes, and what we need now is the full support of as many people as we can get, from every sector possible – including the Chamber!
On that note, I thank you all for listening, and hand you over to Ian to discuss the all-important issue of finance.
Thank you.